
5.0
808+ Reviews
The Cyber Surgery: Benefitting from the ‘Aggregation of Marginal Gains’
Prior to the governing body for professional cycling in Great Britain appointing Sir Dave Brailsford in 2003, British cycling had endured a torrid time. Including nearly 100 years of mediocrity, plus the fact that no British cyclist had ever won cycling’s showpiece, the Tour de France.
In a 10-year span from 2007-2017, under Sir David Brailsford, Great British cycling had what is widely regarded as one of the most successful periods in cycling history. Not only did the previously underwhelming British cyclists win 178 world championships and 66 Olympic or Paralympic gold medals, but during this time they also enjoyed 5 visits to the top step of the podium at the Tour de France.
So how did Brailsford turn around the middling British Cycling and fill our country lanes with MAMILs (Middle aged men in Lycra)? His approach was simple. His belief was that if you improved every facet related to cycling by a mere 1% then the ‘aggregation of marginal gains’ would add up to remarkable improvement.
The First 1% Improvement
I have also found that the ‘aggregation of marginal gains’ has benefits when it comes to dentistry.
Although my journey was somewhat different… as I more stumbled into my aggregation of marginal gains.
In mid-April 2010, I was attending the ITI world symposium in Geneva. The scientific program was divided into three main facets of treatment: New clinical methods for diagnosis and treatment planning; New and proven treatment procedures; Complications in implant dentistry (or dealing with reality!).
My good friend Cyrus Nikkhah was banging on about a new bit of kit from Israel that was going to revolutionise dentistry. This new, interesting technology, called the iTero Intra Oral scanner (IOS), had been acquired by Straumann who had just obtained the European distribution rights.
Despite the scientific committee’s best efforts to sell me on the advantages of intra oral scanning, I still felt unmoved. It wasn’t until Eyjafjallajökull decided to join the party and disrupt air travel that I started to take notice. With no flights and no way to get home, I spent some time playing with the iTero and by the time I managed to get back to blighty (that is a whole story in itself) I had agreed to take one.

Early Tech Adopters
If we weren’t the first practice in the U.K. with an iTero, we must have been the second or third. The remarkable thing too was that this intra-oral scanner was being distributed by an implant company, but it had no way to actually scan the conection of a dental implant, i.e., if you wished to go directly to the implant interface. Therefore, the iTero sat in the corner of the room for a long time, fairly much just gathering dust.
I then rang up Heidi Jeremy at Straumann and said to her that I wanted it to be taken away. That it didn’t work! Heidi asked me if I had actually tried to use it, which was met with a resolute, “Of course!”. Undeterred, Heidi asked the question again. To be met with a less resolute, “Well, it’s slow and it’s scanner is too big” and a few other issues I forget. So, we agreed – that no matter what, I would use it for the next 10 cases that came in the door. It didn’t matter what the case was, whether I was running late, who was assisting me or if the patient had a small mouth. We agreed, and I thought 100%, that I would be giving the scanner back after these 10 cases…
But something happened, by forcing myself to use the scanner. After a small bit of learning about how the technology worked, I went from not using the scanner and looking at it as a bit of junk, to absolutely loving it. Not only did I love it, but so did the patients and the team. So much so that I advised the guys in Harley Street I was working with that in order for me to provide the level of dentistry I wanted to, they would also have to acquire an iTero.


iTero Marginal Gains
So where are the marginal gains? I hear you ask. Well, initially it was as simple as looking at your preparation on a large monitor. One of the first crowns I used the iTero for was on my poor old mum. I was quite happy with my prep until I saw it on the monitor at 60x magnification and then I had to effectively re-prep it as you can’t unsee that sh*t!
So not only did the iTero improve my preparations, but it also led to me getting better loupes. It allowed for ‘impression-making’ rather than ‘impression-taking’, as it was so much easier to add more information if needed, whereas with a conventional impression you just get what you get and adding more detail is usually impossible. Another advantage was somewhat unexpected, the models were amazing! The little articulator that came with them, even though simple, just seemed to work and Rob and Ashley (my technicians) just loved them. Not to mention the bites which seemed better as did the contacts and the fits.

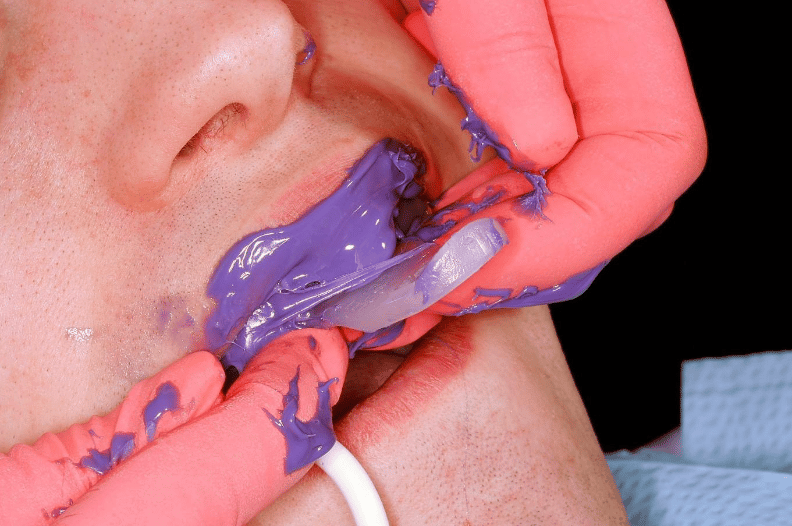
The iTero offered an additional massive benefit, which was that the patients absolutely loved it. Contrary to it being big and bulky, patients preferred it to the gooey impression material. It could be used for patient education, and they were impressed by our adoption of new technology – as many are still today.
Using the Intra Oral Scanner to Scan implants
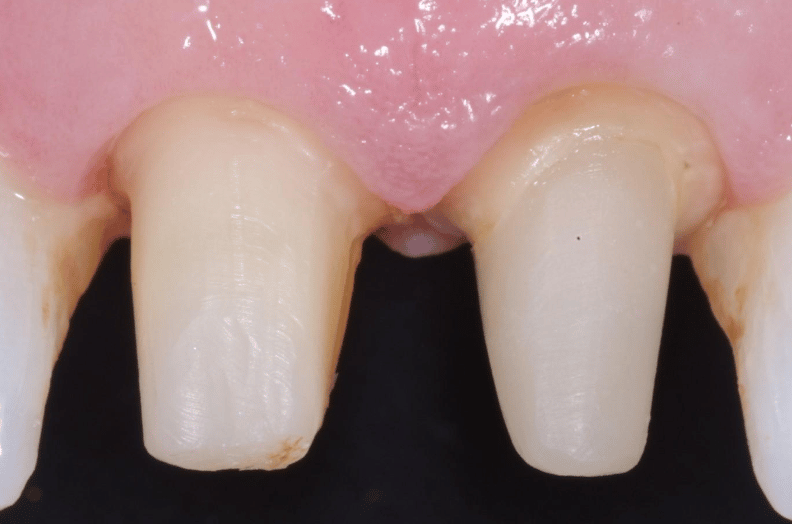
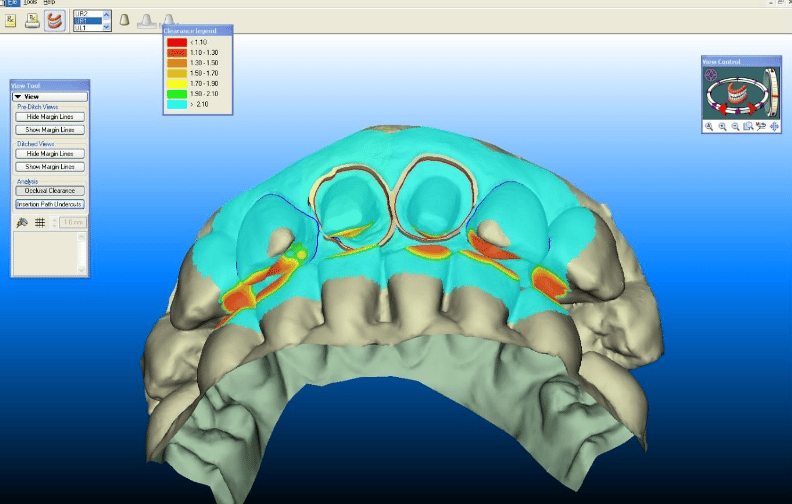
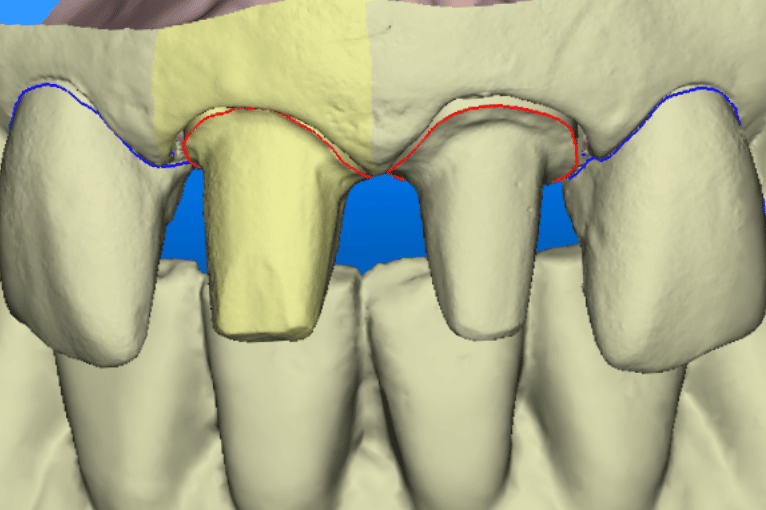
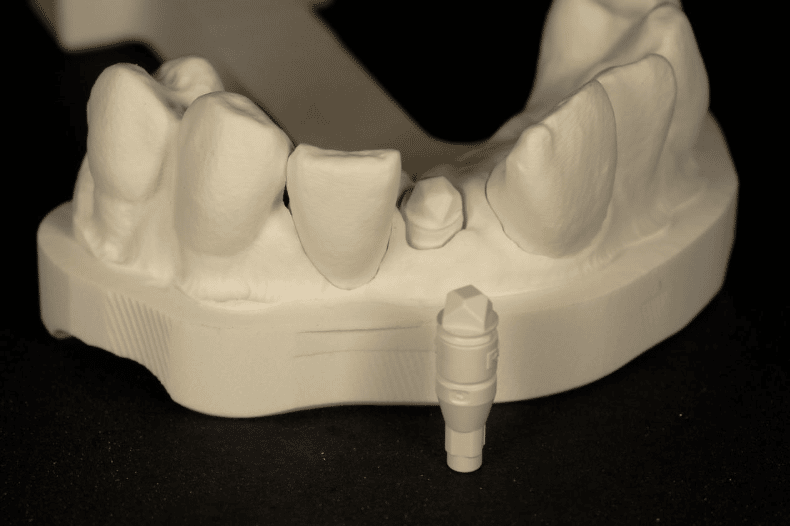
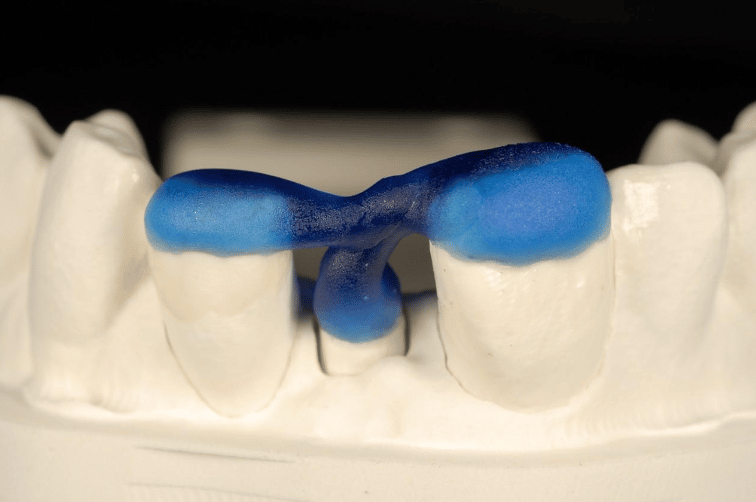
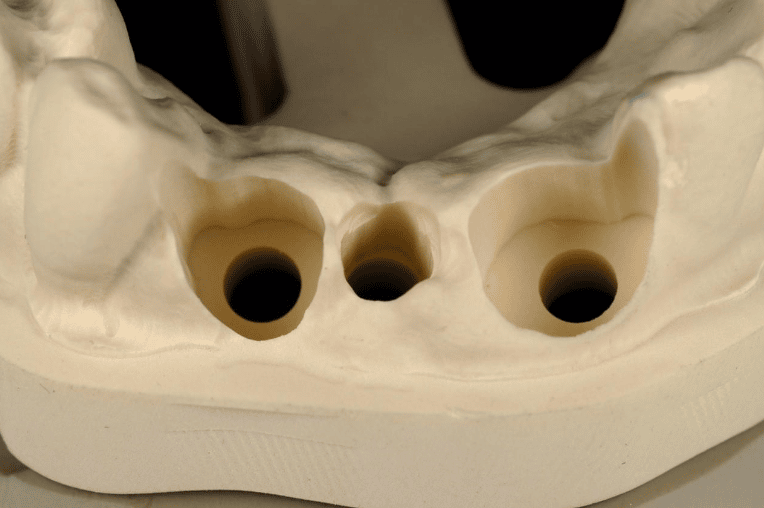
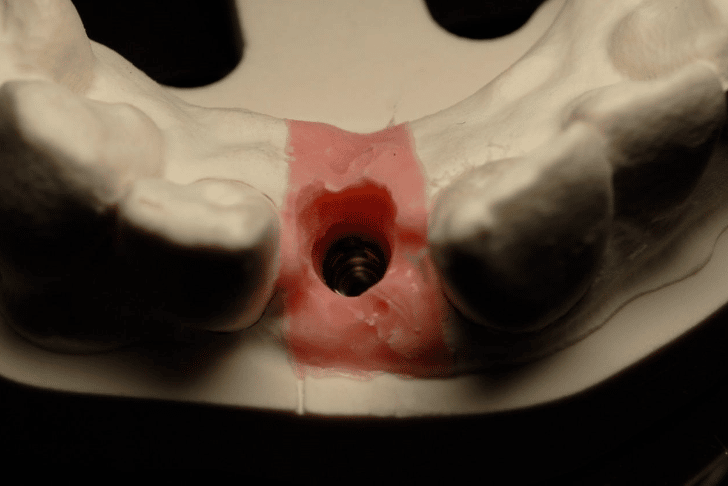
What happens if you have a case like the one below where you have preps and implants? This is an example of a bigger case, one where we wanted to be able to incorporate the fixture position of the implants into the model.

To solve this puzzle, we had to use Kiwi ingenuity. The closest translation of this New Zealand saying would be ‘thinking outside the box’. So that the benefits we were seeing in our conventional workflows could also be applied to our implant cases.
You can see in the series of images below courtesy of Ashley Bryne, how we did this. So now we had the benefits we were seeing with routine work, in our implant cases/combined cases.

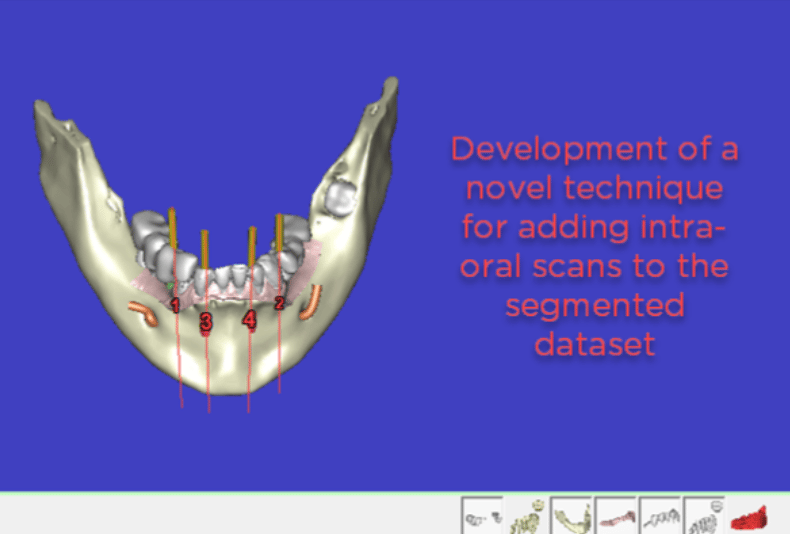
Next Up – The Use of Simplant Imaging
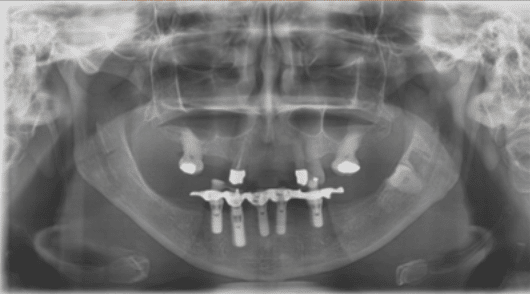
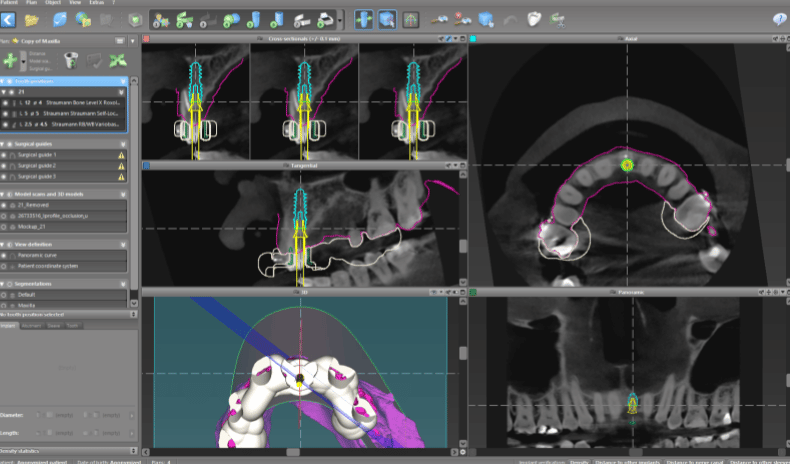
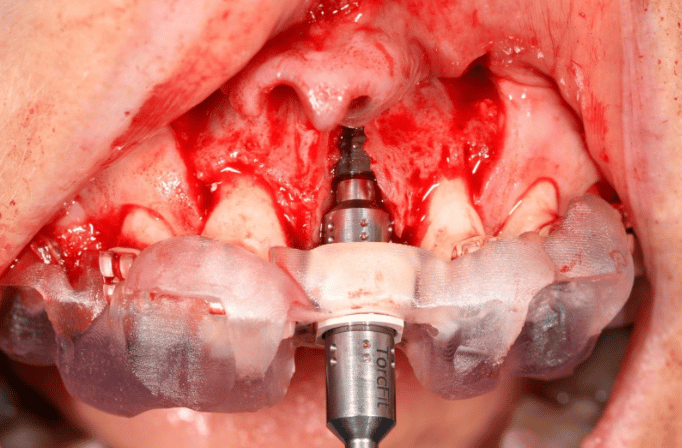
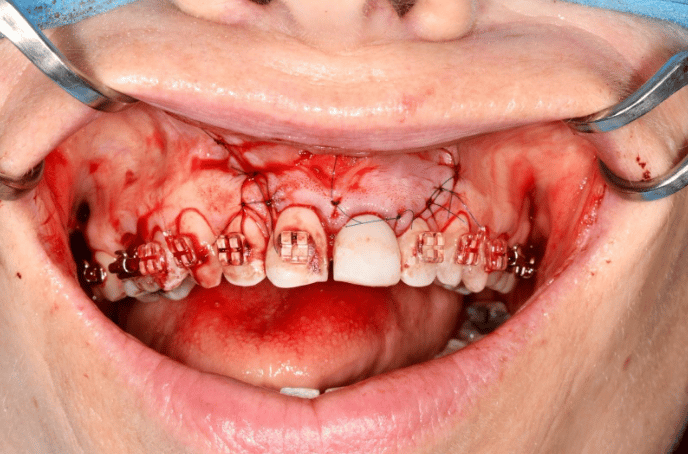
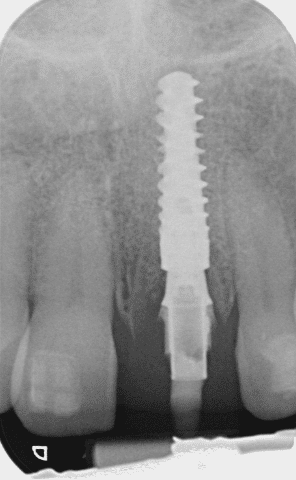
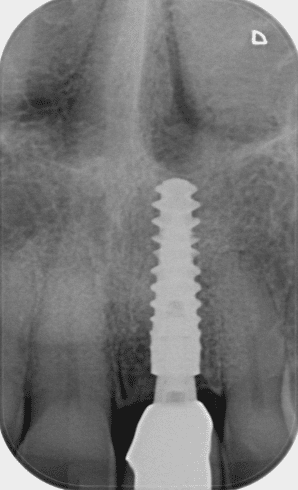
So, what next? We were using Simplant for some of our implant cases, but we felt we were still missing something. So, with the help of Barry Chandler, we started to merge the pre-op intra oral scans with the Simplant planning. It is my understanding that we were the first people to do this in the U.K and possibly Europe. An example of one of the first cases that we did this way is below, including the most recent images of the case. Illustrating the power of guided surgery and constant improvement.
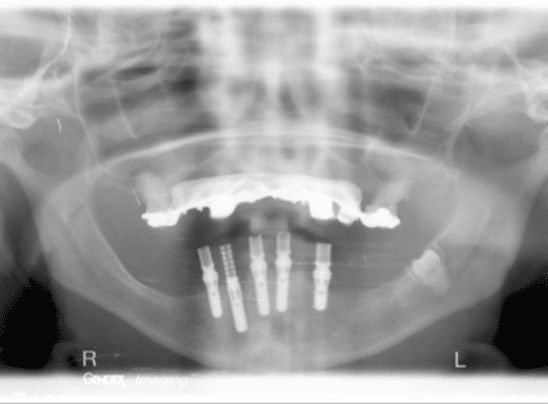

The Sum of Aggregation Over the Years
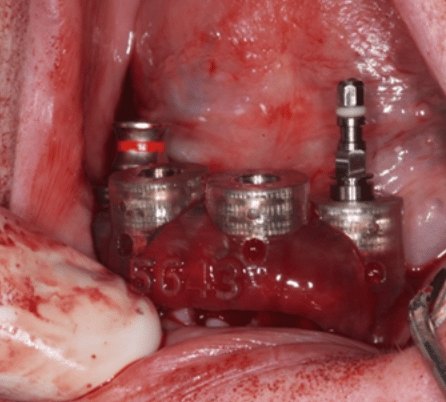
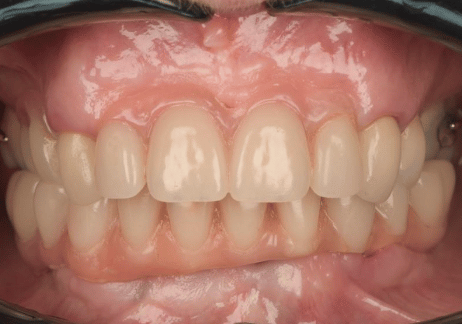
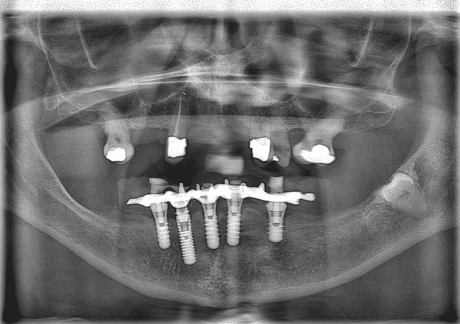
When we jump forward to where we are now, 12 years later, so much has changed with how we provide our implant dentistry. Dare I say it, this is the sum of the aggregation over the years of all of our marginal gains. Not only have we honed our techniques and are using the better, modern equipment available to us, but our systems and processes allow us to work smarter, not harder. Here is a more recent case….






In turn, leaving us time to focus on working on the next 1% improvement.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
You’ve Waited Long Enough
Get in touch with us to learn about award-winning, specialist-led cosmetic, restorative and general services at Reading’s home of slow dentistry.
Get in touch